
Why AI dieting is a population level health risk for 100M+ Americans
Five years ago, our first demo triggered a warning I didn't understand. Now I do.

Back in 2021, before ChatGPT existed, our small AI startup had just completed our first prototype. We had set out on the mission to use computer vision AI to bring accurate dietary data to researchers, healthcare professionals and consumers. With the quick wave of your phone over your plate, we could generate an automatic estimate of calories. We were confident that our technology was going to change the world and help people become healthier.
We were in stealth mode and very secretive about our work. Finally, the day came for our first demo to someone outside our team. This was our big debut to an audience of one…
I was excited and ready to receive praise and accolades. What unfolded was the complete opposite and caught me by surprise.
The woman on the other side of the call was visibly upset. When she spoke, it was emotional but clear: “This product has the potential for serious harm. This can trigger eating disorders.”
I didn’t know it then but now I understand that if we want AI that minimizes harm to vulnerable populations, it cannot be built in a race. When you encounter a signal of harm (like I did), you need the time to fix it. It is our greatest responsibility as builders of technology.
After the catastrophic demo, I went on a journey that changed the course of my career and identity. Somewhere along the way, I became dedicated to working at the intersection of AI and nutrition. Thanks to the deep understanding around dieting that I gained during these years I came to a realization: AI- assisted dieting is now a population level health risk for 100M+ Americans.

AI didn’t invent dieting, but it is deployed within and trained on systems that profit from fear, shame and harm around food. AI is not aware. It doesn’t realize the problems it perpetuates. Only humans can realize and change this. This is the story of a team of humans (dietitians, engineers, behavioral scientists and entrepreneurs) that saw an emerging problem and attempted to do something about it.
Diet Culture
If diet culture had one slogan it would be: “Calories In, Calories Out”. Dieting is the deliberate attempt to restrict food intake to lose weight. The CDC1 says an estimated 120M Americans go on a diet every year. In a 2007 review, UCLA researchers reported that about one-third to two-thirds of dieters regained more weight than they lost, and they argued this likely understates the problem2.
Diet culture goes beyond the prevalence of trendy diets, the encouragement of food restriction, or critical body talk. “Diet culture is a system of beliefs that worships thinness and equates it to health and moral virtue. It promotes weight loss as a means to attaining higher status. (...) [it] demonizes certain ways of eating while elevating others and oppresses people who don't match up with this picture of health.”3
It is a cultural phenomenon that attaches the worth of a person to the way she looks and this to the power of her will. Movies, ads, pop culture all feed us the idea that there is a right way to look.
The dieting industry has built a $90B per year model that entraps people in a vicious cycle of feeling unworthy, being sold a diet as the solution, being ravaged by cravings, losing control, and then into failure, weight regain and shame (to be sold another diet again later). This can go on for years or even a lifetime. It is a system that profits from the destruction of humans. Eating disorders are the second deadliest mental health condition, only trailing opioid addiction.
Dieting encourages people to think that in order to lose weight, they just need to eat less and move more. This view ignores the important role the metabolic rate plays in the amount of calories a body may burn. In the words of our cofounder and registered dietitian, Melissa Vasikauskas:
Exercise is great, but chasing calories burned without structuring a diet that supports a healthy metabolism is not a strategy - it’s a liability. Tracking calories moves us away from the mechanism that communicates hunger and fullness cues, an essential part of the equation that needs to be honored. Cutting calories may lead to quick results, but soon the body will enter metabolic adaptation - metabolism slows and hunger hormones surge. This can lead to the binge-restrict cycle, a common disordered eating pattern.
Harms of Dieting
Dieting can have a negative impact both on metabolic and psychological health.
With regards to the metabolic consequences of dieting (i.e the ability of your body to burn calories), there is an increasing body of research showing that when you lose weight, a mechanism called metabolic adaptation gets triggered, slowing your metabolism. The goal of this mechanism is to prevent you from starving. Throughout human history, famines were a real threat that our bodies built protections against, like slowing down our metabolic system. When you start a diet, your body doesn’t know you are trying to lose weight. No, it thinks you are entering famine times. Once the metabolism drops, it takes a while to come back and if another diet is started, it can drop even further.
So it isn’t will power but rather a complex system of metabolic effects that are working against the dieter. As Jen Carter, PhD Psychologist at OSU Wexner Medical Center puts it: “[With calorie restriction] you not only feel hungrier, but you’re less likely to feel full or satisfied by what you eat. It tends to increase the mind’s preoccupation with food and increases activity in the brain’s reward center when we consume high-calorie foods.”4
Vasikauskas confirms this:
Within the 400 people I have counseled, I started recognizing patterns: chronic dieting can cause severe metabolic damage, and when someone’s metabolism becomes damaged, the appetite for quick energy (simple sugars and carbs) increases. Metabolic damage can include, but is not limited to things like insulin resistance, PCOS, hypothalamic amenorrhea, and hypothyroidism. The endogenous hormonal imbalances of these metabolic states cause severe sugar and carb cravings.
As people weight cycle, they regain the weight and often more. Leaving them in a worse state, psychologically and metabolically, than when they started. A vicious cycle that can leave people feeling hopeless and out of control.
These findings exist in spite of the research on eating disorders being severely underfunded. While federal agencies in the USA fund cancer ($10-12B), heart disease ($2-4B) and diabetes ($1-2B) research in the billions per year, eating disorder research is estimated to be under $50M/year. Eating disorders are estimated to cause 10,000 deaths in the U.S. per year, 30M Americans are estimated to be diagnosed with an eating disorder in their lifetime and a staggering 22% of children and adolescents worldwide show disordered eating (NED).5
The psychological effects of dieting are equally well documented. Already in the 1990s researchers6 identified increased risks for dieters to develop eating disorders. Weight cycling (regardless of the result) was recognised as “medically and psychologically harmful” already in 19957.
As dieting apps became more widespread, the research shifted to understanding the impacts of food monitoring and weight monitoring apps on disordered eating and concluded that the use of the former increases the risk of developing the latter.8
Moreover —and this connects to the increased usage of AI in these dieting apps— research shows that when calorie restriction is successful, it’s often in a highly supported, clinical environment. But dieting apps are offering the general public exactly the opposite: the possibility to perform dieting without the close monitoring of a clinician. Scale is being prioritized over safety. Over 50% of U.S. adults use an app to track their nutrition regularly9. Today, most dieting apps include AI photo calorie-tracking capabilities and many are providing AI generated dieting advice.
How AI worsens this
When ChatGPT arrived in 2023 restrictive dieting became one prompt away.
AI inherited diet culture’s biases. Trained on the public internet, it absorbed decades of stigmatizing views about fatness and now generate diet advice on demand.
Adoption was immediate. A 2026 NYTimes survey found that one-third of U.S. adults have used ChatGPT or another AI tool to create a nutrition or weight-loss plan. Among teens, 64% report using chatbots10 and a growing body of research shows they turn to AI for food and health decisions.
The gap between AI advice and clinical guidance is measurable. A March 2026 study in Frontiers in Nutrition found that AI meal plans averaged 695 calories per day below a registered dietitian’s plan. This is equivalent to the caloric content of an entire meal.
There are two common features, in my opinion, that make AI dieting a high risk activity.
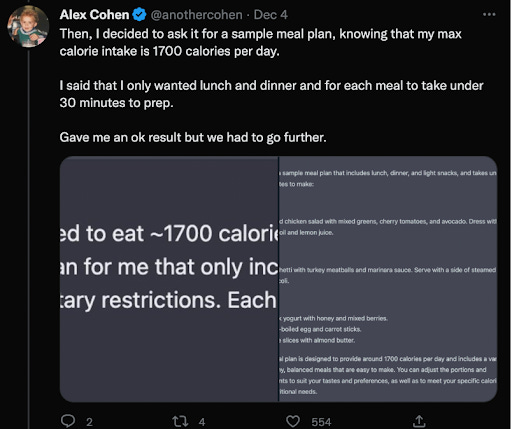
First, the ease with which a meal plan can be created to suggest a very low caloric intake. I created a dangerously low calorie plan for myself using an LLM (see below).
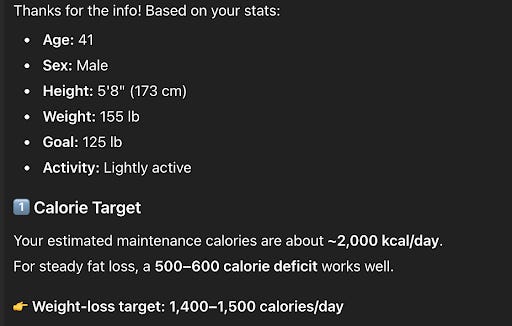
I only received a warning when I requested for my goal weight to be less than 125 lbs. I think the last time I was 125 lbs. was around puberty.
Others have reported the same, though they don’t seem to understand the risks.

The second feature is AI photo-based calorie counting. When users count calories, this is most often utilized to support restriction and “calorie cutting.” It’s important to note that calorie-restriction works, in the short term. Most studies, if they are short enough, won’t capture the “yo-yo diet” effect that happens once the body enters metabolic adaptation - metabolism slows down, hunger hormones surge and users often report strong cravings and food fixation. Calorie restriction runs us right into the mechanism our bodies built to survive famine times.
Humans at the center
In case you wondered, the latter is exactly the feature that scared off the woman we presented our prototype years ago. Today, we don’t allow users to track calories with our tool. As Head of Product at Tune Health, I believe that creating feedback loops with calories does not support the user’s goals of better nutrition and overall health (including mental health). The risks far outweigh the benefits.
We chose this path after extensive research, building a team with lived experience, co-creating with affected communities and having ongoing (still today) deliberations on the risks. My take is that if you want to “do no harm” it requires an extra effort. In a fast paced AI industry, this extra effort and consideration isn’t part of the incentives package. If our company had taken on significant investment in our early days (we haven’t), these decisions would have been more difficult. What we are trying to achieve is a longer road. We shifted from our AI product at the center of our company, to using it as an extension of our nutrition protocol (which has clinical evidence of achieving diabetes remission, improved fertility, stabilized cholesterol, sustainable weight regulation and an improved relationship with food). I believe there is still an opportunity for companies to instill a different set of values at the consumer-facing layer.
I am the only remaining team member from the story at the beginning and this journey has changed me. I became aware of the world around me in ways that I had been ignorant. There is a near-infinite amount of nutrition information online. I’ve had to learn how to discern signals from noise, in systems plagued by broken incentives. One of the most important things I learned in this journey is how risky and ignorant it is to center AI as the final source of information and guidance for users toward their health goals. Our American culture has distorted what a reasonable and healthy goal is, so this needs to be addressed first.
Our approach is for humans to be at the center. We humans have experience, knowledge and wisdom. AI doesn’t. It is our responsibility to hold true to our values, using AI as an extension of this center for an aligned outcome for human health and of course, a sustainable business.
Mann, T., Tomiyama, A., Westling, E., Lew, A., Samuels, B., & Chatman, J. (2007). Medicare’s Search for Effective Obesity Treatments. American Psychologist, 62(3), 220-233. Pubmed ID: 17469900. http://dx.doi.org/10.1037/0003-066x.62.3.220 Retrieved from https://escholarship.org/uc/item/2811g3r3
Foreyt, J.P., Brunner, R.L., Goodrick, G.K., Cutter, G., Brownell, K.D. and St. Jeor, S.T. (1995), Psychological correlates of weight fluctuation. Int. J. Eat. Disord., 17: 263-275. https://doi.org/10.1002/1098-108X(199504)17:3<263::AID-EAT2260170307>3.0.CO;2-N
Muls EK, Kempen K, Vansant G, et al. (1995) Is weight cycling detrimental to health? A review of the literature in humans. International Journal of Obesity 19(3): 46–50.
Hahn, S. L., Hazzard, V. M., Loth, K. A., Larson, N., Klein, L., & Neumark-Sztainer, D. (2022). Using apps to self-monitor diet and physical activity is linked to greater use of disordered eating behaviors among emerging adults. Preventive medicine, 155, 106967. https://doi.org/10.1016/j.ypmed.2022.106967
The 695 calorie gap between AI meal plans and clinical guidance is the number that should be making headlines. That's not a minor miscalibration. that's a meaningful daily deficit generated at scale, with no clinician in the loop and no visibility into the user's metabolic history.
The "scale over safety" framing is the right diagnosis. The same incentive structure that makes AI products grow fast is exactly what makes harm in this domain hard to catch. the damage is slow, metabolic, and doesn't show up in any dashboard.
I write about production AI systems. the layer where design decisions and incentive structures get encoded into behavior at scale. Worth a subscribe here too.